심한 출혈은 병원에 도착한 뒤 시작되는 문제가 아니다. 몇 분의 지연이 생명을 가르는 순간, 지혈 기술은 곧 생존 기술이 된다. 적혈구를 서로 단단히 연결하는 ‘클릭 혈전’ 연구는 피를 멈추는 방식을 새롭게 상상하게 한다.
[Key Message]
* 출혈은 병원에 도착한 뒤가 아니라, 사고가 발생한 바로 그 순간부터 생명을 위협한다. 따라서 지혈 기술은 단순한 응급 처치가 아니라, 환자에게 치료받을 시간을 벌어주는 생존 기술이다.
* ‘클릭 혈전’ 기술은 피가 자연스럽게 굳기를 기다리는 대신, 적혈구 표면 단백질을 연결해 인공 혈전을 빠르게 만드는 새로운 접근이다. 이는 혈액을 수동적인 치료 대상이 아니라, 상처를 막는 생체 재료로 활용한다는 점에서 의미가 크다.
* 몇 초 만에 형성되는 인공 혈전은 응급실, 수술실, 구급차, 재난 현장, 전장 의료에서 중요한 가능성을 가진다. 특히 심각한 외상이나 대량 출혈처럼 시간이 생명을 좌우하는 상황에서 새로운 지혈 도구가 될 수 있다.
* 강한 혈전은 생명을 구할 수 있지만, 동시에 원치 않는 혈전 형성이라는 위험도 안고 있다. 따라서 실제 의료 현장에 적용되기 위해서는 독성, 면역반응, 혈관 막힘, 분해 과정, 장기 안전성에 대한 엄격한 검증이 필요하다.
* 이 연구의 의미는 단순히 피를 빨리 멈추는 데 있지 않다. 혈액세포와 생체재료를 설계해 몸 안에서 필요한 구조물을 만드는 미래 의학의 방향을 보여준다는 점에서 더 큰 의미가 있다.
***
생명을 가르는 첫 몇 분
사람의 몸은 놀라울 만큼 정교하게 설계되어 있다. 피부가 찢어지고 혈관이 손상되면, 몸은 즉시 피를 멈추기 위한 복구 작업을 시작한다. 혈소판이 상처 부위에 달라붙고, 응고 단백질이 차례로 작동하며, 섬유소가 그물처럼 얽혀 혈액을 붙잡는다. 우리가 흔히 ‘피가 굳는다’고 말하는 과정 뒤에는 사실 수많은 세포와 단백질, 신호 물질이 동원되는 복잡한 생명 현상이 숨어 있다.
하지만 이 정교한 시스템에도 약점이 있다. 너무 큰 상처 앞에서는 시간이 부족하다. 작은 상처라면 몸의 자연 응고 과정이 충분히 작동할 수 있지만, 간이나 대동맥 주변의 손상, 총상, 교통사고, 산업재해, 수술 중 대량 출혈처럼 피가 빠르게 빠져나가는 상황에서는 몸이 혈전을 만들기도 전에 생명이 위태로워진다. 출혈은 단순히 피가 흐르는 현상이 아니라, 산소를 나르는 혈액이 몸 밖으로 빠져나가면서 장기와 뇌가 버틸 시간을 잃어가는 과정이다.
응급의료에서 출혈은 늘 시간과의 싸움이었다. 구급대원이 현장에 도착하기 전까지, 환자가 병원으로 이송되는 동안, 수술실에서 손상 부위를 찾아내기 전까지, 의료진이 할 수 있는 가장 중요한 일은 피가 더 이상 빠져나가지 않게 붙잡는 것이다. 그래서 압박붕대, 지혈대, 거즈, 수술용 접착제, 혈액응고제, 수혈은 오랫동안 응급의료의 기본 장비가 되어왔다. 문제는 이 장비들이 모든 상황에서 충분히 빠르고 강하게 작동하지는 않는다는 점이다.
피가 흐르는 속도가 빠르고 상처가 깊으면, 단순히 표면을 덮는 것만으로는 부족하다. 상처 안쪽에서 계속 피가 밀려나오면 지혈 물질이 떨어져 나가거나 씻겨 내려갈 수 있다. 혈액이 잘 굳지 않는 환자라면 자연 응고 과정 자체가 늦거나 불안정할 수 있다. 항응고제를 복용 중인 고령자, 혈우병 같은 응고장애 환자, 외상으로 체온과 혈압이 급격히 떨어진 환자에게는 작은 출혈도 심각한 위기로 번질 수 있다. 결국 지혈 기술의 핵심은 단순하다. 얼마나 빨리, 얼마나 단단하게, 얼마나 안전하게 피를 멈출 수 있는가.
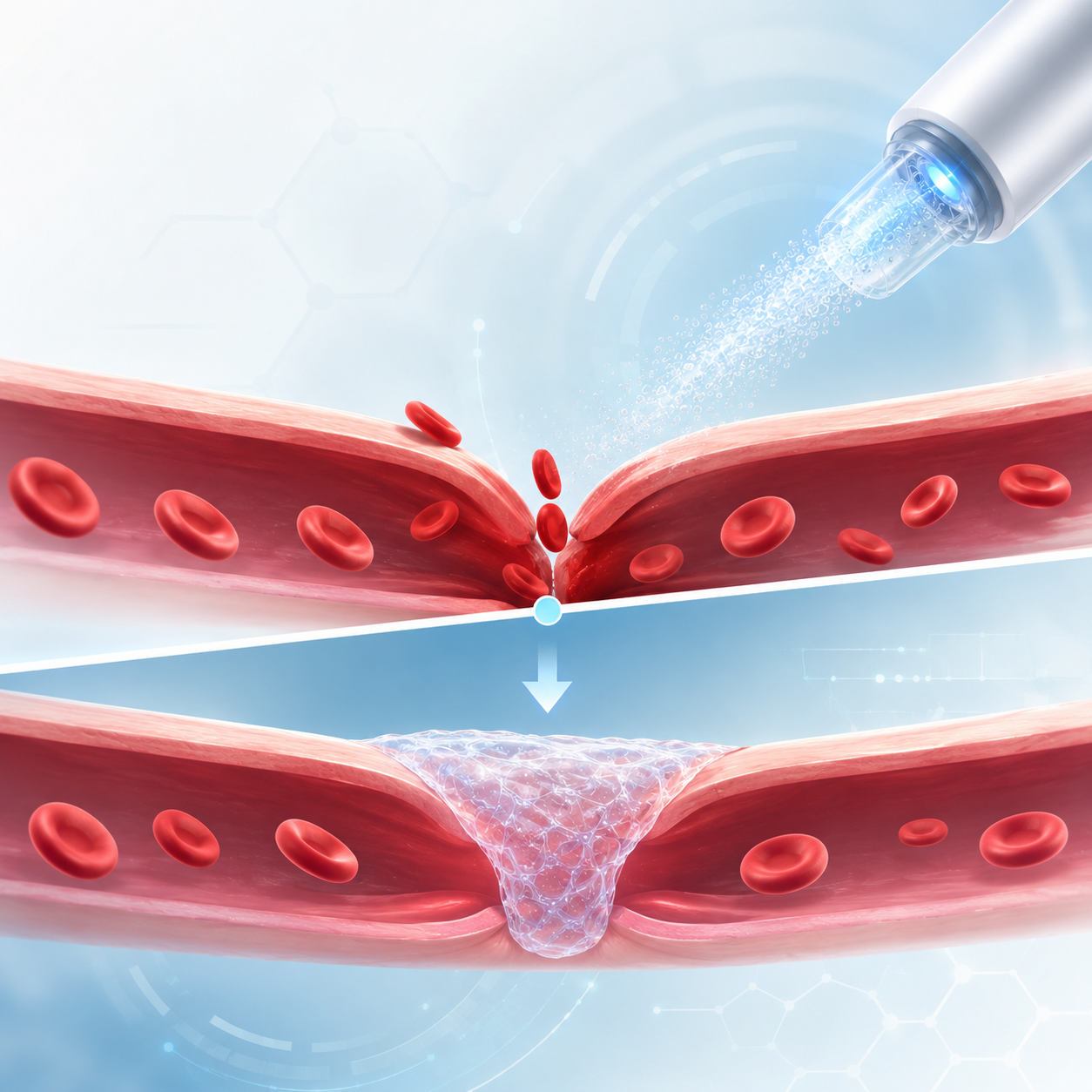
이 질문 앞에서 최근 주목받은 연구가 있다. 국제 학술지 Nature에 2026년 4월 29일 소개된 ‘클릭 혈전’ 연구다. 맥길대 연구진은 적혈구 표면 단백질을 빠른 화학반응으로 서로 연결해, 몇 초 안에 단단한 인공 혈전 형태의 겔을 만드는 방식을 제시했다. 이 기술은 자연 혈전보다 파열에 강하고, 조직에 더 잘 달라붙는 성질을 보였으며, 쥐 실험에서는 심각한 출혈을 빠르게 막을 가능성을 확인했다. 연구진은 이 접근이 응급의료, 상처 치료, 응고장애 치료에 활용될 수 있다고 설명했다.
중요한 것은 ‘인공 혈전’이라는 표현이 주는 낯섦보다 그 발상의 전환이다. 그동안 지혈은 몸이 스스로 혈전을 만들도록 돕거나, 상처를 바깥에서 눌러 막는 방식에 가까웠다. 그런데 이번 연구는 혈액 안에 이미 존재하는 적혈구를 구조물의 재료로 삼는다. 피가 멈추기를 기다리는 것이 아니라, 피 자체를 빠르게 붙잡아 상처를 막는 재료로 바꾸려는 시도다. 지혈의 무대가 붕대와 거즈의 표면에서, 혈액 속 세포의 표면으로 이동한 셈이다.
피를 기다리는 의학에서 피를 설계하는 의학으로
우리는 혈액을 대체로 ‘흐르는 액체’로 생각한다. 산소를 나르고, 영양분을 전달하고, 노폐물을 치우는 붉은 액체. 하지만 출혈이 일어나는 순간 혈액은 다른 얼굴을 드러낸다. 흐르던 혈액은 멈춰야 하고, 액체였던 피는 상처를 막는 임시 구조물로 바뀌어야 한다. 이 전환의 중심에 혈전이 있다. 혈전은 몸이 스스로 만드는 생체 접착제이자 임시 방벽이다.
자연 혈전의 기본 구조는 혈소판과 섬유소, 그리고 혈액세포들이 함께 얽힌 덩어리다. 혈소판은 손상 부위에 빠르게 모여들어 초기 마개를 만들고, 섬유소는 그 마개를 더 튼튼하게 고정한다. 적혈구는 그 사이에 갇히면서 혈전의 부피와 형태에 영향을 준다. 전통적으로 적혈구는 산소를 운반하는 세포로 주로 이해되었다. 혈전 안에서도 어느 정도는 ‘채워지는 재료’에 가까운 존재로 여겨졌다. 하지만 최근 생체재료 연구는 적혈구를 더 적극적인 구조 재료로 바라보기 시작했다.
클릭 혈전 연구의 흥미로운 지점도 여기에 있다. 연구진은 적혈구를 단순히 혈전 안에 갇히는 세포가 아니라, 서로 연결될 수 있는 미세한 건축 자재처럼 다룬다. 적혈구 표면에는 여러 단백질이 존재한다. 이 단백질들을 빠르고 생체친화적인 화학반응으로 연결하면, 각각 떠다니던 적혈구들이 서로 맞물려 하나의 겔 구조를 만들 수 있다. 마치 흩어진 벽돌들이 순간적으로 접착되어 단단한 벽을 이루는 것과 비슷하다.
여기서 ‘클릭’이라는 표현은 우연히 붙은 이름이 아니다. 화학에서 클릭 반응은 비교적 빠르고 선택적으로 일어나며, 복잡한 생체 환경에서도 원하는 분자끼리 잘 연결되도록 설계된 반응을 가리킬 때 쓰인다. 일상적인 비유로 말하면, 레고 블록이 딱 맞물리듯 두 분자가 빠르게 결합하는 방식이다. 연구진은 이 원리를 혈액 속 적혈구 표면에 적용했다. 그 결과 적혈구들이 서로 연결되면서 단단한 겔 형태의 인공 혈전, 즉 ‘Cyto-Gel’이 만들어진다.
이 발상은 기존 지혈제와 다르다. 기존 지혈 물질은 대개 상처 표면을 덮거나, 응고 과정을 촉진하거나, 피를 흡수해 굳게 만드는 방식이었다. 물론 이런 기술도 중요하다. 실제 의료 현장에서는 지혈 거즈, 피브린 글루, 트롬빈 기반 제제, 콜라겐 스펀지, 산화셀룰로오스 등 다양한 지혈 재료가 사용된다. 하지만 큰 출혈이나 압력이 높은 출혈에서는 물질이 상처에 오래 붙어 있어야 하고, 혈액의 흐름을 견뎌야 하며, 손상 조직과 잘 접착해야 한다. 단순히 ‘응고를 촉진한다’는 것만으로는 충분하지 않은 순간이 있다.
클릭 혈전은 바로 이 지점에서 새로운 가능성을 제시한다. 혈액 속 세포를 서로 연결해, 상처 부위에서 물리적으로 더 튼튼한 덩어리를 만들 수 있다면, 출혈을 막는 방식이 달라질 수 있다. 자연 혈전이 만들어지기까지의 시간을 줄이고, 만들어진 혈전이 흐름과 압력에 버티는 힘을 높이는 것이다. 연구진이 보고한 수치도 이 점을 잘 보여준다. 실험에서 인공 혈전은 자연 혈전보다 파열 저항성이 13배 높고, 접착력은 4배 강한 것으로 소개됐다.
물론 이 수치만으로 당장 임상 적용을 말할 수는 없다. 실험실에서 강한 구조를 보이는 것과 사람의 몸 안에서 안전하게 작동하는 것은 다른 문제다. 하지만 방향은 분명하다. 지혈 기술은 이제 단순히 상처를 막는 재료를 찾는 단계에서, 혈액세포와 단백질의 결합 방식을 설계하는 단계로 나아가고 있다. 피는 더 이상 수동적인 치료 대상만이 아니다. 피 안의 세포 자체가 치료 재료가 될 수 있다.
5초 만에 만들어지는 작은 방벽
이 연구가 대중적으로 강한 인상을 주는 이유는 ‘5초’라는 시간 때문이다. 의학 연구에는 복잡한 수치와 개념이 많지만, 5초라는 시간은 누구나 직관적으로 이해할 수 있다. 상처가 난 뒤 손으로 누를 틈도 없이 피가 솟구치는 장면, 수술 중 예기치 못한 출혈이 발생한 순간, 전장에서 부상자가 쓰러진 뒤 구급 처치가 시작되는 순간을 떠올려보면 5초는 결코 짧은 숫자가 아니다. 그 짧은 시간 안에 피를 붙잡을 수 있다면, 생명을 구할 수 있는 창이 넓어진다.
클릭 혈전의 작동 방식은 겉으로는 단순해 보인다. 적혈구 표면의 단백질을 화학적으로 연결한다. 그렇게 연결된 적혈구들은 서로 엉겨 붙어 겔처럼 변한다. 이 겔은 상처 부위에 붙어 피가 더 이상 빠져나가지 못하도록 막는다. 하지만 그 안에는 여러 층의 기술적 의미가 있다. 첫째, 반응은 빠르게 일어나야 한다. 둘째, 혈액과 조직에 닿아도 독성이 낮아야 한다. 셋째, 혈액의 자연 응고 과정과 완전히 충돌하지 않아야 한다. 넷째, 형성된 구조물은 흐르는 피의 압력을 견딜 만큼 튼튼해야 한다.
이 네 가지 조건을 동시에 만족시키는 일은 쉽지 않다. 너무 강한 화학반응은 세포를 손상시킬 수 있다. 너무 느린 반응은 응급 상황에서 의미가 떨어진다. 너무 약한 구조는 출혈 압력을 견디지 못한다. 너무 오래 남는 물질은 회복 과정에 방해가 될 수 있다. 생체재료 연구가 어려운 이유가 여기에 있다. 몸 안에서 쓰이는 재료는 단단하기만 해서도 안 되고, 부드럽기만 해서도 안 된다. 필요할 때는 강하게 버티고, 시간이 지나면 몸의 회복 과정과 조화를 이루어야 한다.
연구진은 클릭 혈전이 자연 혈전과 함께 작동할 수 있다는 점도 강조했다. 인공 혈전이 몸의 응고 과정을 완전히 대체하는 것이 아니라, 자연 혈전이 형성되는 환경 속에서 더 튼튼한 구조를 제공하는 방식이다. 보도 내용에 따르면 이 겔은 피브린과 통합될 수 있으며, 손상된 간 출혈 모델에서 지혈과 조직 재생 가능성을 보였다. 큰 틀에서 보면 이것은 ‘대체’보다 ‘보강’에 가까운 전략이다. 몸의 자연 복구 과정을 없애는 것이 아니라, 그 과정이 너무 느리거나 약할 때 구조적 지지대를 제공하는 것이다.
쥐 실험에서 간 손상을 대상으로 했다는 점도 중요하다. 간은 혈류가 풍부한 장기다. 한 번 손상되면 출혈이 많고, 지혈이 쉽지 않다. 외상이나 수술에서 간 출혈은 의료진에게 큰 부담이 되는 상황 중 하나다. 따라서 간 손상 모델에서 빠른 지혈 가능성을 보였다는 것은 기술의 잠재력을 설명하기에 좋은 단서가 된다. 다만 동물실험에서의 성공은 어디까지나 초기 가능성이다. 사람의 몸은 크기와 혈류, 면역반응, 기저질환, 약물 복용 상태가 훨씬 다양하다. 실험실과 임상 사이에는 늘 긴 검증의 다리가 놓여 있다.
그럼에도 ‘5초의 혈전’이라는 개념은 강력하다. 응급의료의 세계에서는 몇 초가 치료의 성패를 가를 때가 많다. 심정지 환자에게 가슴압박이 늦어지는 몇 분, 뇌졸중 환자가 혈관 재개통 치료를 받기까지의 시간, 외상 환자의 대량 출혈이 조절되기까지의 시간이 모두 생존율과 후유증에 영향을 준다. 그런 점에서 클릭 혈전은 단지 새로운 지혈제가 아니라, 응급의학이 가장 두려워하는 ‘시간의 공백’을 줄이려는 기술로 읽힌다.
응급실과 구급차 사이의 빈틈
의료기술은 대개 병원 안에서 빛난다. 고성능 영상장비, 수술로봇, 중환자실, 정밀진단, 맞춤형 약물치료는 모두 병원이라는 공간에서 작동한다. 그러나 생명을 위협하는 출혈은 병원 밖에서 시작되는 경우가 많다. 도로 위 사고 현장, 공장 바닥, 산악 구조 현장, 재난 지역, 전장, 외딴 지역의 보건소, 구급차 안에서 먼저 벌어진다. 응급의료의 가장 큰 어려움은 바로 이 간극이다. 가장 정교한 치료는 병원에 있지만, 가장 급한 순간은 병원에 도착하기 전에 찾아온다.
그래서 지혈 기술의 진짜 가치는 현장성에서 드러난다. 아무리 뛰어난 지혈 물질이라도 보관이 어렵고, 사용 절차가 복잡하고, 전문 장비가 필요하면 현장에서 쓰기 어렵다. 반대로 조금 덜 정교하더라도 빠르게 꺼내 쓸 수 있고, 다양한 상처에 적용 가능하며, 온도와 이동 조건을 견딜 수 있다면 응급현장에서 큰 의미를 가진다. 클릭 혈전이 실제 기술로 발전하려면 이 질문을 피할 수 없다. 몇 초 안에 겔이 만들어지는 것만큼이나, 그 겔을 어떻게 준비하고, 어떻게 보관하고, 누가 어떤 절차로 사용할 것인가가 중요하다.
보도에 따르면 연구진은 환자 자신의 혈액을 활용하는 자가 방식과, 혈액형이 맞는 기증 혈액을 활용하는 동종 방식의 가능성을 모두 언급했다. 자가 방식은 환자 자신의 혈액을 쓰기 때문에 면역반응이나 거부반응 부담을 줄일 수 있지만, 준비 시간이 더 걸릴 수 있다. 동종 방식은 미리 준비된 혈액을 바탕으로 더 빠르게 쓸 수 있지만, 혈액형과 보관, 안전성 관리가 중요해진다. 관련 보도에서는 동종 방식은 10분 이내, 자가 방식은 약 20분 정도의 준비 가능성이 언급됐다.
이 지점은 매우 현실적이다. 흔히 ‘5초 만에 혈전이 생긴다’고 하면 마치 주사기 하나로 모든 출혈을 즉시 막을 수 있을 것처럼 상상하기 쉽다. 그러나 실제 의료기술은 준비, 보관, 적용, 사후 관리까지 포함한 전체 시스템으로 평가된다. 응급실에서는 10분도 빠른 시간일 수 있지만, 전장이나 재난 현장에서는 10분이 길게 느껴질 수 있다. 구급차 안에서는 채혈과 조작이 가능할 수도 있지만, 사고 현장 한복판에서는 어려울 수도 있다. 따라서 클릭 혈전의 미래는 화학반응의 속도뿐 아니라 의료 시스템 안에서 얼마나 간단한 형태로 구현되느냐에 달려 있다.
만약 이 기술이 안정화된다면 가장 먼저 떠올릴 수 있는 현장은 외상센터다. 외상 환자는 피를 많이 흘린 채 병원에 도착하는 경우가 많고, 의료진은 손상 부위를 찾고 수술을 준비하는 동안 출혈을 조절해야 한다. 다음은 수술실이다. 간, 비장, 혈관, 심장 주변 수술처럼 출혈 위험이 큰 수술에서는 지혈재의 성능이 수술 시간을 줄이고 합병증을 낮추는 데 영향을 줄 수 있다. 또 하나는 응고장애 환자다. 혈액이 잘 굳지 않는 환자에게 강한 생체재료 기반 지혈제가 도움이 될 가능성이 있다.
전장 의료에서도 의미가 크다. 전쟁터에서 가장 치명적인 부상 가운데 하나는 대량 출혈이다. 병원으로 이송되기 전, 제한된 장비와 인력으로 피를 막아야 하는 상황이 많다. 최근 군 의료는 지혈대, 압박 드레싱, 지혈 거즈 같은 현장형 기술을 꾸준히 발전시켜왔다. 여기에 더 강하고 빠른 인공 혈전 기술이 결합된다면, 전장 부상자의 생존 가능성을 높이는 새로운 도구가 될 수 있다. 물론 군사적 활용 가능성은 윤리적 질문도 함께 낳는다. 생명을 구하는 기술은 전장에서도 필요하지만, 전쟁의 지속 가능성을 높이는 기술로만 소비되어서는 안 된다.
응급의료의 관점에서 클릭 혈전은 하나의 기술인 동시에 하나의 방향이다. 병원 안에서만 작동하는 고급 치료가 아니라, 병원 밖의 첫 순간까지 확장되는 치료. 몸의 자연 회복을 기다리는 것이 아니라, 그 회복이 시작될 수 있도록 시간을 벌어주는 치료. 가장 위험한 순간에 의료진에게 몇 분의 여유를 만들어주는 치료. 지혈 기술이 바뀐다는 것은 단순히 상처 치료법이 바뀐다는 뜻이 아니다. 생명을 구할 수 있는 공간이 병원 밖으로 넓어진다는 뜻이다.
강한 혈전이 던지는 불편한 질문
그러나 혈전을 강하게 만든다는 말은 동시에 조심스러운 말이다. 혈전은 생명을 구하기도 하지만, 생명을 위협하기도 한다. 상처 부위에서 피를 막는 혈전은 필요하지만, 혈관 안에서 원치 않게 생기는 혈전은 뇌졸중, 심근경색, 폐색전 같은 치명적인 질환으로 이어질 수 있다. 같은 단어가 상황에 따라 치료가 되기도 하고 재난이 되기도 한다. 그래서 인공 혈전 기술은 기대만큼이나 엄격한 안전성 검증이 필요하다.
가장 먼저 확인해야 할 것은 위치의 문제다. 인공 혈전은 반드시 필요한 상처 부위에서만 작동해야 한다. 겔이 상처를 막은 뒤 일부가 떨어져 혈류를 타고 이동하면 문제가 될 수 있다. 혈관을 막는 색전이 되지 않는지, 작은 조각으로 분해될 때 안전한지, 몸 안에서 얼마나 오래 남는지, 어떤 방식으로 제거되는지 확인해야 한다. 지혈제는 강해야 하지만, 무작정 강해서는 안 된다. 피를 멈춘 뒤에는 회복 과정과 함께 적절히 사라져야 한다.
둘째는 면역반응이다. 적혈구는 원래 몸 안에 존재하는 세포지만, 표면 단백질이 화학적으로 연결되거나 변형되면 몸이 이를 어떻게 인식할지 알 수 없다. 자가 혈액을 쓰면 부담이 줄어들 수 있지만, 응급 상황에서는 항상 자가 방식이 가능하지 않을 수 있다. 기증 혈액을 사용할 경우 혈액형, 감염 위험, 보관 안정성, 면역 적합성 문제가 따라온다. 연구진은 동물실험에서 주요 장기 독성이나 위험한 면역반응의 징후를 보지 못했다고 보도됐지만, 사람에게 적용하려면 훨씬 넓고 긴 검증이 필요하다.
셋째는 응고 시스템과의 상호작용이다. 사람의 혈액응고 과정은 복잡하다. 항응고제를 복용하는 환자, 간질환 환자, 암 환자, 고령자, 임산부, 중증 외상 환자처럼 응고 상태가 달라진 사람들에게 같은 물질이 같은 방식으로 작동하지 않을 수 있다. 어떤 환자에게는 충분히 강하지 않을 수 있고, 어떤 환자에게는 과도하게 작동할 수 있다. 지혈 기술은 평균적인 몸이 아니라, 실제 응급실에 오는 다양한 몸을 상대로 검증되어야 한다.
넷째는 회복의 문제다. 좋은 지혈제는 피를 멈추는 데서 끝나지 않는다. 상처가 아물 수 있는 환경을 만들어야 한다. 너무 딱딱한 물질이 조직 사이에 오래 남으면 회복을 방해할 수 있고, 염증을 유발할 수도 있다. 반대로 너무 빨리 사라지면 다시 출혈이 발생할 수 있다. 클릭 혈전 연구가 조직 재생 가능성까지 언급되는 이유는 바로 이 부분 때문이다. 지혈과 재생은 분리된 과정이 아니다. 피를 멈추는 순간부터 몸은 손상된 조직을 복구하기 시작한다. 지혈 재료가 이 복구 과정에 방해가 되지 않고 오히려 돕는다면, 그 가치는 훨씬 커진다.
이런 질문들은 연구의 의미를 깎아내리는 것이 아니다. 오히려 기술이 실제 의료로 나아가기 위해 반드시 통과해야 할 관문이다. 초기 연구에서 중요한 것은 가능성의 문을 여는 일이다. 그 다음 단계는 안전성, 반복성, 제조 표준화, 대량 생산, 보관, 규제 승인, 임상시험이다. 한 번의 논문이 곧바로 치료제가 되는 것은 아니다. 특히 혈액과 응고에 관련된 기술은 작은 변수도 큰 결과를 만들 수 있기 때문에 더 보수적으로 검증되어야 한다.
그럼에도 이 연구가 흥미로운 이유는 분명하다. 위험을 감수하자는 이야기가 아니라, 위험을 이해하면서도 지혈 기술의 한계를 넘어설 새로운 길을 보여주기 때문이다. 현재 의료 현장에도 많은 지혈제가 있지만, 심각한 출혈은 여전히 생명을 위협한다. 완벽한 기술이 없기 때문에 새로운 접근이 필요하다. 클릭 혈전은 그 접근 가운데 하나다. 적혈구를 단순한 산소 운반 세포가 아니라, 필요한 순간 상처를 막는 구조 재료로 바꿀 수 있다는 상상력. 바로 그 상상력이 이 연구의 가장 큰 힘이다.
피 한 방울에 담긴 생체재료 혁명
클릭 혈전은 지혈 기술이지만, 더 넓게 보면 생체재료 기술의 한 장면이다. 생체재료란 몸 안팎에서 조직, 세포, 장기와 접촉하며 치료를 돕는 재료를 말한다. 인공관절, 심장 스텐트, 봉합사, 인공피부, 약물전달 젤, 조직공학용 지지체가 모두 이 범주에 들어간다. 과거의 생체재료는 주로 몸에 ‘들어가도 큰 문제가 없는’ 재료를 찾는 데 집중했다. 몸이 거부하지 않고, 독성이 낮고, 오래 버티는 재료가 중요했다. 하지만 최근의 생체재료는 더 적극적으로 변하고 있다. 몸 안에서 특정 반응을 일으키고, 세포의 행동을 조절하며, 조직 재생을 유도하는 ‘작동하는 재료’로 진화하고 있다.
클릭 혈전도 이런 흐름 안에 있다. 단순히 상처 위에 얹는 물질이 아니라, 혈액 속 세포와 반응해 새로운 구조를 만드는 재료다. 피가 흐르는 환경, 세포 표면, 단백질 결합, 조직 접착, 응고 과정이 모두 연결된다. 이 기술이 중요한 이유는 적혈구라는 익숙한 세포를 새로운 방식으로 활용한다는 데 있다. 우리는 적혈구를 너무 잘 안다고 생각하지만, 생명과학은 익숙한 대상에서 계속 새로운 기능을 발견한다. 산소 운반 세포였던 적혈구가, 이제는 생체 구조물의 중심 재료로 다시 해석되고 있다.
이 변화는 의료기술 전반의 흐름과도 맞닿아 있다. 현대 의학은 점점 더 ‘정적인 물질’에서 ‘동적인 시스템’으로 이동하고 있다. 약은 단순히 몸에 들어가 작용하는 화학물질이 아니라, 특정 세포와 조직을 겨냥하는 정밀한 신호가 되고 있다. 인공장기는 단순한 대체물이 아니라, 세포와 재료가 함께 살아 움직이는 구조로 발전하고 있다. 의료용 접착제도 단순히 붙이는 풀을 넘어, 젖은 조직과 혈액 속에서도 작동하고 분해되는 스마트 소재로 바뀌고 있다.
출혈을 멈추는 기술도 마찬가지다. 과거의 지혈은 ‘누르고 막는’ 기술에 가까웠다. 앞으로의 지혈은 ‘붙고, 버티고, 통합되고, 회복을 돕는’ 기술이 될 가능성이 크다. 상처 부위에서 혈액세포를 구조화하고, 섬유소와 결합하며, 조직에 접착하고, 시간이 지나면 몸의 회복 과정 속으로 흡수되는 재료. 이것은 더 이상 단순한 지혈제가 아니다. 응급의학, 재생의학, 재료공학, 혈액학이 만나는 융합 기술이다.
특히 혈액은 접근성이 높은 생체 재료다. 환자의 몸에서 비교적 쉽게 얻을 수 있고, 이미 몸 안에서 중요한 기능을 수행하는 세포와 단백질을 포함하고 있다. 만약 혈액을 현장에서 빠르게 가공해 치료 재료로 바꿀 수 있다면, 의료의 많은 장면이 달라질 수 있다. 환자 자신의 혈액으로 상처를 막고, 조직 회복을 돕고, 약물을 전달하는 방식이 더 정교해질 수 있다. 물론 이를 위해서는 자동화된 장비, 표준화된 제조 공정, 안전한 반응 조건이 필요하다. 하지만 방향은 분명하다. 몸의 재료를 몸의 치료에 다시 쓰는 의학이다.
여기서 중요한 것은 기술의 화려함보다 의료 접근성이다. 고급 기술이 일부 대형병원에만 머물면 생명을 구할 수 있는 범위가 제한된다. 반대로 안전하고 간단하며 휴대 가능한 형태로 발전한다면, 응급의료의 격차를 줄이는 도구가 될 수 있다. 시골 지역, 재난 현장, 전장, 개발도상국의 의료 현장처럼 수혈과 수술 접근성이 낮은 곳에서 빠른 지혈 기술은 더 큰 의미를 갖는다. 생체재료 혁명은 실험실의 논문으로 끝나지 않는다. 가장 취약한 현장에서 쓸 수 있을 때 비로소 의료 혁신이 된다.
이번 연구가 던지는 메시지는 그래서 더 넓다. 피는 단순한 액체가 아니다. 피 안에는 산소 운반, 면역, 응고, 회복이라는 생명의 기본 기능이 담겨 있다. 그 기능을 이해하고, 필요한 순간에 정교하게 조정할 수 있다면, 우리는 몸 안의 재료를 활용해 더 빠르고 강한 치료를 설계할 수 있다. 클릭 혈전은 그 가능성을 보여주는 작은 창이다.
전장 의료와 재난 의료가 주목하는 이유
새로운 지혈 기술이 등장할 때마다 군 의료와 재난 의료가 관심을 갖는 이유는 명확하다. 가장 위험한 출혈은 대개 가장 열악한 환경에서 발생한다. 폭발 사고, 총상, 교통사고, 건물 붕괴, 산업재해, 자연재해에서는 출혈이 심하지만 의료자원은 부족하다. 응급실처럼 조명이 밝고 장비가 갖춰진 공간이 아니라, 먼지와 소음, 혼란 속에서 처치가 이루어진다. 의료진은 많지 않고, 환자는 여러 명이며, 이송 시간은 길다. 이런 환경에서는 빠르고 강한 지혈 기술이 곧 생존율을 바꿀 수 있다.
전장 의료의 역사는 지혈 기술 발전의 역사이기도 하다. 과거에는 지혈대 사용이 오히려 조직 손상을 키울 수 있다는 우려로 제한적으로 쓰이기도 했다. 하지만 대량 출혈을 막지 못해 사망하는 사례가 반복되면서, 현대 전장 의료에서는 적절한 지혈대 사용이 중요한 생존 처치로 자리 잡았다. 지혈 거즈와 압박 드레싱도 같은 이유로 발전했다. 이 기술들은 모두 병원 밖에서 피를 멈추기 위한 도구다. 클릭 혈전이 실제 현장형 기술로 발전한다면, 이 계보의 다음 단계가 될 수 있다.
물론 전장 적용을 상상할 때는 과장을 경계해야 한다. 클릭 혈전이 곧바로 병사 개인의 구급낭에 들어갈 수 있다는 뜻은 아니다. 보관 조건, 준비 과정, 주입 방식, 부작용 관리, 훈련 수준이 모두 해결되어야 한다. 혈액 기반 기술이라면 냉장 보관이나 혈액형 관리가 필요할 수 있고, 화학반응을 이용한다면 사용 절차가 표준화되어야 한다. 전장에서는 작은 실수도 큰 위험으로 이어질 수 있다. 따라서 군 의료에서 실제로 쓰이려면 기술은 극도로 단순하고 견고해야 한다.
재난 의료에서도 마찬가지다. 대형 사고가 발생하면 병원 시스템은 한꺼번에 밀려드는 환자들로 압박을 받는다. 이때 현장에서 출혈을 조절할 수 있으면 중증 환자를 병원까지 살려 보낼 가능성이 커진다. 특히 복부나 흉부 내부 출혈처럼 밖에서 압박하기 어려운 출혈은 여전히 큰 문제다. 인공 혈전 기술이 언젠가 주입형, 패치형, 겔형 등 다양한 형태로 발전한다면, 압박이 어려운 상처에서도 새로운 대안이 될 수 있다.
수술실도 중요한 적용 영역이다. 외상 수술이나 장기 절제 수술에서는 피를 멈추는 데 걸리는 시간이 수술 전체의 안정성을 좌우한다. 출혈이 계속되면 시야가 흐려지고, 수혈량이 늘고, 환자의 체온과 응고 기능이 악화된다. 지혈이 빨라지면 수술 시간과 합병증을 줄일 가능성이 있다. 이미 수술실에는 다양한 지혈제가 있지만, 더 강하고 조직 접착력이 높은 재료는 늘 필요하다. 클릭 혈전이 기존 제품보다 더 우수한 성능을 보였다는 초기 결과는 그래서 주목된다.
하지만 가장 중요한 질문은 ‘누구에게 먼저 필요한가’다. 이 기술은 모든 상처에 필요한 기술이 아니다. 종이에 손을 베인 상처나 작은 외상에는 기존 지혈로 충분하다. 클릭 혈전 같은 기술이 의미를 갖는 곳은 생명이 위험한 출혈, 자연 응고가 부족한 환자, 수술 중 조절이 어려운 출혈, 기존 지혈제로 충분하지 않은 상황이다. 기술의 가치를 제대로 평가하려면 적용 대상을 정확히 좁혀야 한다. 모든 문제를 해결하는 만능 지혈제가 아니라, 가장 위험한 출혈 상황에서 시간을 벌어주는 고성능 도구로 보는 것이 현실적이다.
그런 점에서 이 연구는 응급의료의 미래를 생각하게 한다. 앞으로 응급 처치는 단순히 환자를 병원으로 옮기는 일이 아니라, 병원에 도착하기 전부터 고급 치료의 일부를 시작하는 방향으로 갈 가능성이 크다. 휴대용 초음파, 현장 혈액검사, 원격의료, 드론 배송, 인공지능 환자 분류, 자동 주입 장치 같은 기술이 이미 응급의료의 경계를 바꾸고 있다. 클릭 혈전 같은 지혈 기술이 여기에 결합되면, 병원 밖 의료의 수준은 더 높아질 수 있다. 생명을 살리는 첫 치료가 병원 문턱이 아니라 사고 현장에서 시작되는 것이다.
기술의 미래는 속도보다 신뢰에 달려 있다
클릭 혈전 연구를 바라볼 때 가장 경계해야 할 태도는 두 가지다. 하나는 지나친 낙관이다. ‘5초 만에 피를 멈춘다’는 표현은 강렬하지만, 아직 사람에게 널리 쓰이는 치료제가 된 것은 아니다. 동물실험과 초기 생체재료 연구는 가능성을 보여주는 단계다. 실제 임상 적용까지는 많은 시간이 필요하다. 안전성, 유효성, 제조 공정, 규제 승인, 비용, 의료 현장 적용성까지 검증해야 한다. 과학의 세계에서 가능성은 출발점이지 결승선이 아니다.
다른 하나는 지나친 냉소다. 아직 초기 연구라는 이유만으로 의미를 작게 볼 필요도 없다. 의료 혁신은 대개 이런 작은 개념 전환에서 시작된다. 처음에는 실험실의 겔이고, 동물실험의 결과이며, 제한된 조건에서의 수치다. 하지만 그 안에 새로운 원리가 있다면, 후속 연구는 그 원리를 더 안전하고 실용적인 형태로 다듬어간다. 혈액세포를 구조 재료로 활용한다는 발상은 충분히 강한 연구적 의미를 가진다. 그것이 곧바로 치료제가 되지 않더라도, 지혈 기술의 방향을 넓히는 데 기여할 수 있다.
미래의 지혈 기술은 몇 가지 방향으로 발전할 가능성이 있다. 첫째, 더 빠른 준비다. 응급현장에서 쓰려면 혈액을 채취하고 반응시키는 과정이 간단해야 한다. 둘째, 더 안전한 분해다. 피를 멈춘 뒤 몸 안에서 어떻게 사라지는지 예측 가능해야 한다. 셋째, 더 정밀한 위치 제어다. 상처 부위에서만 작동하고 혈관 내부의 불필요한 응고를 유발하지 않아야 한다. 넷째, 다양한 형태다. 주입형, 패치형, 스프레이형, 수술용 겔형 등 현장과 상처의 종류에 맞게 달라질 수 있다. 다섯째, 비용과 보급성이다. 고가의 특수 치료에 머물지 않고 실제 응급의료 시스템에 들어갈 수 있어야 한다.
여기서 신뢰가 중요해진다. 생명을 다루는 기술은 놀라운 속도보다 신뢰할 수 있는 반복성이 더 중요하다. 한 번 성공한 실험보다, 수천 번의 다양한 조건에서 비슷하게 작동하는 안정성이 필요하다. 젊고 건강한 실험동물보다, 실제 환자처럼 복잡한 몸에서 안전하게 작동해야 한다. 피를 멈추는 기술은 응급 상황에서 쓰이기 때문에, 의료진이 망설이지 않고 사용할 수 있어야 한다. 기술이 아무리 뛰어나도 현장에서 믿고 쓸 수 없다면 생명을 구하는 도구가 되기 어렵다.
또한 윤리적 질문도 따라온다. 혈액 기반 생체재료를 만들 때 기증 혈액을 어떻게 사용할 것인가. 응급 상황에서 환자의 동의를 어떻게 다룰 것인가. 전장 의료에 쓰이는 기술이 민간 의료로도 충분히 확산될 것인가. 고가 기술이 일부 국가와 병원에만 집중되지 않을 것인가. 응급의료 기술은 생명과 직결되기 때문에, 접근성과 공정성의 문제를 피할 수 없다. 좋은 기술은 단지 강한 성능을 가진 기술이 아니라, 필요한 사람에게 도달할 수 있는 기술이어야 한다.
한국의 의료 환경에서도 이 주제는 의미가 있다. 한국은 외상센터 체계를 강화해왔지만, 중증 외상 환자의 이송과 초기 처치, 지역 간 의료 격차는 여전히 중요한 문제다. 고령화가 진행될수록 항응고제를 복용하는 환자도 늘고, 낙상이나 사고 뒤 출혈 관리가 더 중요해진다. 산업 현장과 군 의료, 도서산간 응급의료에서도 빠른 지혈 기술은 관심을 가질 만한 영역이다. 클릭 혈전이 당장 한국 의료 현장에 도입된다는 뜻은 아니지만, 차세대 응급의료 기술이 어디로 향하는지 보여주는 신호로 볼 수 있다.
결국 이 연구의 진짜 의미는 하나의 제품보다 더 넓다. 피를 멈추는 방식이 바뀌고 있다. 몸이 스스로 혈전을 만들기를 기다리는 의학에서, 혈액세포의 표면을 설계해 필요한 순간 강한 구조물을 만드는 의학으로 이동하고 있다. 상처를 덮는 물질에서, 상처 안에서 작동하는 생체재료로 이동하고 있다. 응급의료는 더 빠르고, 더 현장 가까이 가고, 더 정밀해질 것이다.
5초라는 시간은 짧다. 하지만 그 5초 안에는 긴 질문이 들어 있다. 피를 얼마나 빨리 멈출 수 있는가. 멈춘 피가 다시 흐르지 않도록 얼마나 단단히 붙잡을 수 있는가. 그 과정이 몸에 얼마나 안전한가. 그리고 이 기술이 실제 현장의 환자에게 얼마나 가까이 갈 수 있는가. 클릭 혈전 연구는 이 질문들에 대한 첫 답을 보여준다. 아직 완성된 치료는 아니지만, 분명한 방향은 제시한다.
출혈을 막는 일은 오래전부터 의학의 가장 기본적인 과제였다. 인간은 상처를 누르고, 묶고, 꿰매고, 약을 바르며 피를 멈추려 했다. 이제 그 오래된 과제 앞에 새로운 도구가 등장하고 있다. 적혈구를 연결해 만든 인공 혈전. 몇 초 만에 형성되는 작은 생체 방벽. 그것은 단순한 실험실의 신기술이 아니라, 응급의료가 생명과 시간을 다루는 방식을 바꿀 수 있는 가능성이다.
피를 멈추는 기술은 결국 시간을 되찾는 기술이다. 환자가 병원에 도착할 시간, 의료진이 손상 부위를 찾을 시간, 몸이 회복을 시작할 시간, 생명이 다시 버틸 시간을 만들어주는 기술이다. 클릭 혈전이 아직 넘어야 할 검증의 문은 많지만, 그 문 너머에는 분명 새로운 의료의 풍경이 있다. 피가 흐르는 순간, 의학은 더 이상 기다리기만 하지 않는다. 이제 의학은 피 안의 세포를 붙잡아, 생명을 지키는 벽을 세우려 한다.
Reference
Nature. “Engineered blood clots stop bleeding in seconds.” April 29, 2026.
Nature. “Synthetic blood clots snap cells together to staunch bleeding — fast.” April 29, 2026.
McGill University. “McGill researchers engineer faster, more effective blood clots.” April 29, 2026.
The Five-Second Technology That Stops Bleeding
- Artificial Blood Clots Are Changing the Timeframe of Emergency Medicine
Severe bleeding is not a problem that begins only after a patient reaches the hospital. When a delay of just a few minutes can decide life or death, hemostatic technology becomes a technology of survival. Research on “click clotting,” which tightly links red blood cells together, invites us to imagine a new way of stopping blood loss.
[Key Messages]
* Severe bleeding threatens life from the very moment an accident occurs, not only after a patient reaches the hospital. Hemostatic technology is therefore not just emergency treatment, but a survival technology that buys patients the time they need to receive care.
* Click clotting offers a new approach by rapidly creating artificial clots through the linking of proteins on the surface of red blood cells, instead of waiting for blood to clot naturally. Its significance lies in treating blood not as a passive target of treatment, but as a biological material that can help seal wounds.
* Artificial clots that form within seconds could have major potential in emergency rooms, operating rooms, ambulances, disaster sites, and battlefield medicine. They may become a new hemostatic tool in situations where time determines survival, such as severe trauma or massive bleeding.
* Stronger clots can save lives, but they also carry the risk of unwanted clot formation. Before this technology can be used in real medical settings, strict verification is needed for toxicity, immune response, vascular blockage, degradation, and long-term safety.
* The significance of this research is not limited to stopping bleeding quickly. It points toward a future of medicine in which blood cells and biomaterials are engineered to create necessary structures inside the body.
***
The First Few Minutes That Decide Life
The human body is astonishingly sophisticated. When the skin is torn and a blood vessel is damaged, the body immediately begins repair work to stop the bleeding. Platelets attach to the wound site, clotting proteins activate in sequence, and fibrin becomes entangled like a net to hold the blood in place. Behind what we casually call “blood clotting” lies a complex biological process involving countless cells, proteins, and signaling molecules.
But even this sophisticated system has a weakness. In the face of a major wound, there is not enough time. For a small injury, the body’s natural clotting process may work well enough. But in cases such as liver injury, damage near major arteries, gunshot wounds, traffic accidents, industrial injuries, or massive bleeding during surgery, life may be endangered before the body has time to form a clot. Bleeding is not simply the visible flow of blood. It is the process by which oxygen-carrying blood leaves the body, while the organs and brain gradually lose the time they need to survive.
In emergency medicine, bleeding has always been a race against time. Before paramedics arrive at the scene, while the patient is being transported to the hospital, and before surgeons can locate the damaged area in the operating room, the most important thing medical teams can do is prevent further blood loss. That is why compression bandages, tourniquets, gauze, surgical adhesives, clotting agents, and transfusions have long been basic tools of emergency care. The problem is that these tools do not always work quickly or strongly enough in every situation.
When blood is flowing rapidly and the wound is deep, simply covering the surface is not enough. If blood continues to push out from inside the wound, hemostatic materials can detach or be washed away. If the patient’s blood does not clot well, the natural clotting process itself may be delayed or unstable. In elderly patients taking anticoagulants, in people with clotting disorders such as hemophilia, or in trauma patients whose body temperature and blood pressure have dropped sharply, even a relatively small bleed can become a serious crisis. In the end, the central question of hemostatic technology is simple. How quickly, how firmly, and how safely can bleeding be stopped?
A recent study has drawn attention in response to this question. It is the study on “click clotting,” introduced in Nature on April 29, 2026. Researchers at McGill University proposed a method for creating a firm artificial blood-clot-like gel within seconds by linking proteins on the surface of red blood cells through a rapid chemical reaction. The technique showed greater resistance to rupture and stronger adhesion to tissue than natural clots, and mouse experiments confirmed its potential to stop severe bleeding quickly. The researchers explained that this approach could be used in emergency medicine, wound treatment, and the treatment of clotting disorders.
What matters is not the unfamiliarity of the phrase “artificial blood clot,” but the shift in thinking behind it. Until now, hemostasis has largely meant helping the body make its own clot or stopping the wound externally by pressure. This study, however, uses red blood cells already present in the blood as structural material. Instead of waiting for bleeding to stop, it attempts to turn the blood itself into a material that can rapidly hold itself together and seal the wound. In that sense, the stage of hemostasis has moved from the surface of bandages and gauze to the surface of cells inside the blood.
From Medicine That Waits for Blood to Medicine That Designs Blood
We usually think of blood as a flowing liquid. A red fluid that carries oxygen, delivers nutrients, and removes waste. But the moment bleeding occurs, blood reveals another face. Blood that had been flowing must stop, and what had been a liquid must transform into a temporary structure that seals the wound. At the center of this transition is the blood clot. A clot is the body’s biological adhesive and temporary barrier.
The basic structure of a natural clot is a mass in which platelets, fibrin, and blood cells become entangled. Platelets quickly gather at the damaged site to form an initial plug, and fibrin secures that plug more firmly. Red blood cells become trapped inside the structure and influence the clot’s volume and shape. Traditionally, red blood cells have mainly been understood as cells that carry oxygen. Even within a clot, they were often regarded as something close to a filler material. But recent biomaterials research has begun to see red blood cells as more active structural components.
The interesting point of click clotting research lies here. The researchers treat red blood cells not as cells that are merely trapped inside a clot, but as tiny building materials that can be linked together. Various proteins exist on the surface of red blood cells. If these proteins are connected through fast and biocompatible chemical reactions, individual red blood cells floating separately can interlock and form a single gel structure. It is similar to scattered bricks being instantly bonded together to form a solid wall.
The word “click” was not chosen by chance. In chemistry, a click reaction refers to a reaction that occurs relatively quickly and selectively, and is often designed so that desired molecules can connect well even in complex biological environments. In everyday terms, it is like two molecules snapping together the way Lego blocks fit into place. The researchers applied this principle to the surface of red blood cells in the bloodstream. As a result, the red blood cells became linked together, forming a firm gel-like artificial clot called “Cyto-Gel.”
This idea differs from conventional hemostatic agents. Existing hemostatic materials usually cover the wound surface, promote clotting, or absorb blood to help it solidify. These technologies are, of course, important. In actual medical settings, various hemostatic materials are used, including hemostatic gauze, fibrin glue, thrombin-based agents, collagen sponges, and oxidized cellulose. But in cases of major bleeding or high-pressure bleeding, the material must remain attached to the wound, withstand the flow of blood, and adhere well to damaged tissue. There are moments when simply “promoting clotting” is not enough.
Click clotting presents a new possibility at precisely this point. If blood cells can be linked together to create a physically stronger mass at the wound site, the way we stop bleeding could change. The aim is to shorten the time it takes for a natural clot to form and to increase the strength with which the clot withstands flow and pressure. The figures reported by the researchers illustrate this point well. In experiments, the artificial clot was reported to be thirteen times more resistant to rupture and four times more adhesive than a natural clot.
Of course, these numbers alone do not mean that clinical use is immediately possible. A structure that appears strong in the laboratory and a material that works safely inside the human body are two different things. But the direction is clear. Hemostatic technology is moving beyond the search for materials that simply seal wounds. It is advancing toward the design of how blood cells and proteins connect. Blood is no longer only a passive target of treatment. The cells within blood itself may become therapeutic materials.
A Small Barrier Formed in Five Seconds
The reason this research makes such a strong public impression is the time: five seconds. Medical research often contains complex figures and concepts, but five seconds is a period anyone can understand intuitively. Imagine a wound from which blood spurts before a hand can even press down, an unexpected bleed during surgery, or the moment a wounded person collapses on a battlefield and emergency care begins. In those moments, five seconds is not a trivial number. If blood can be held in place within that brief span, the window for saving a life widens.
The mechanism of click clotting looks simple from the outside. Proteins on the surface of red blood cells are chemically linked. The linked red blood cells then clump together and become gel-like. This gel attaches to the wound site and prevents more blood from escaping. But inside that apparently simple process are several layers of technical meaning. First, the reaction must occur quickly. Second, it must have low toxicity when it touches blood and tissue. Third, it must not completely interfere with the body’s natural clotting process. Fourth, the structure that forms must be strong enough to withstand the pressure of flowing blood.
Satisfying all four conditions at once is not easy. A chemical reaction that is too strong can damage cells. A reaction that is too slow loses meaning in an emergency. A structure that is too weak cannot withstand the pressure of bleeding. A material that remains too long in the body can interfere with recovery. This is why biomaterials research is difficult. A material used inside the body cannot be merely hard or merely soft. It must hold strongly when needed and then harmonize with the body’s recovery process over time.
The researchers also emphasized that click clots can work together with natural clots. The artificial clot does not completely replace the body’s clotting process. Instead, it provides a stronger structure within the environment where a natural clot is forming. According to reports, the gel can integrate with fibrin and showed potential for both hemostasis and tissue regeneration in a damaged liver bleeding model. In broad terms, this is a strategy of reinforcement rather than replacement. It does not remove the body’s natural repair process; it provides structural support when that process is too slow or too weak.
The fact that the mouse experiments used liver injury as a model is also important. The liver is an organ rich in blood flow. Once it is damaged, bleeding can be heavy and difficult to control. In trauma or surgery, liver bleeding is one of the situations that places a heavy burden on medical teams. Therefore, showing the possibility of rapid hemostasis in a liver injury model is a meaningful clue to the technology’s potential. Still, success in animal experiments remains an early sign of possibility. The human body is far more diverse in size, blood flow, immune response, underlying disease, and medication use. Between the laboratory and the clinic there is always a long bridge of verification.
Even so, the concept of a “five-second clot” is powerful. In emergency medicine, a few seconds can often decide the outcome of treatment. The minutes lost before chest compressions begin in cardiac arrest, the time before a stroke patient receives vascular reopening treatment, and the time it takes to control massive bleeding in trauma all affect survival and long-term disability. In that sense, click clotting is not merely a new hemostatic agent. It is a technology aimed at narrowing the “gap of time” that emergency medicine fears most.
The Gap Between the Emergency Room and the Ambulance
Medical technology usually shines inside the hospital. High-performance imaging equipment, surgical robots, intensive care units, precision diagnostics, and customized drug treatments all operate within the space of the hospital. But life-threatening bleeding often begins outside the hospital. It first occurs on a road after a crash, on the floor of a factory, at a mountain rescue site, in a disaster zone, on a battlefield, in a rural clinic, or inside an ambulance. This gap is one of the greatest difficulties in emergency medicine. The most sophisticated treatment is in the hospital, but the most urgent moment arrives before the patient reaches it.
That is why the real value of hemostatic technology is revealed in the field. No matter how excellent a hemostatic material may be, it is difficult to use on site if it is hard to store, complicated to apply, or requires specialized equipment. By contrast, even if a technology is somewhat less sophisticated, it can have enormous value in emergency settings if it can be used quickly, applied to various wounds, and withstand temperature and transport conditions. If click clotting is to develop into a real technology, it cannot avoid this question. Just as important as forming a gel within seconds is how that gel is prepared, stored, and used, and by whom.
According to reports, the researchers mentioned the possibility of both an autologous method using the patient’s own blood and an allogeneic method using donor blood with a matching blood type. The autologous method can reduce concerns about immune reactions or rejection because it uses the patient’s own blood, but it may take longer to prepare. The allogeneic method can be used more quickly based on preprepared blood, but blood type, storage, and safety management become important. Related reports mentioned that the allogeneic method could be prepared within ten minutes, while the autologous method may take about twenty minutes.
This point is very realistic. When people hear that “a clot forms in five seconds,” it is easy to imagine that a single syringe could instantly stop every bleed. But real medical technology is evaluated as a whole system that includes preparation, storage, application, and follow-up care. In an emergency room, ten minutes may be fast, but on a battlefield or at a disaster site, ten minutes can feel long. In an ambulance, blood collection and handling may be possible, but in the middle of an accident scene, it may not be. Therefore, the future of click clotting depends not only on the speed of the chemical reaction, but also on how simply it can be implemented within medical systems.
If this technology becomes stable, the first place that comes to mind is the trauma center. Trauma patients often arrive at the hospital after losing large amounts of blood, and medical teams must control bleeding while locating the injury and preparing for surgery. The next place is the operating room. In surgeries with a high risk of bleeding, such as those involving the liver, spleen, blood vessels, or regions near the heart, the performance of hemostatic materials can influence surgical time and complications. Another possible area is patients with clotting disorders. A strong biomaterial-based hemostatic agent may help patients whose blood does not clot well.
Battlefield medicine is another area where the implications are significant. One of the deadliest injuries in war is massive bleeding. In many situations, bleeding must be stopped with limited equipment and personnel before the injured person can be transported to a hospital. Modern military medicine has steadily developed field-based technologies such as tourniquets, compression dressings, and hemostatic gauze. If a stronger and faster artificial clotting technology is added to this set of tools, it could become a new way to improve the survival of battlefield casualties. Of course, possible military use also raises ethical questions. Technologies that save lives are needed even on the battlefield, but they should not be consumed only as tools that make war more sustainable.
From the perspective of emergency medicine, click clotting is both a single technology and a broader direction. It points toward treatment that works not only within the hospital but extends to the first critical moments outside it. It is treatment that does not simply wait for the body’s natural recovery, but buys time so that recovery can begin. It gives medical teams a few extra minutes in the most dangerous moments. A change in hemostatic technology does not merely mean a change in wound care. It means the space in which lives can be saved may expand beyond the hospital.
The Uncomfortable Questions Raised by Stronger Clots
However, the idea of making clots stronger must be approached carefully. Blood clots can save lives, but they can also threaten lives. A clot that stops bleeding at a wound site is necessary, but a clot that forms where it is not wanted inside a blood vessel can lead to fatal conditions such as stroke, myocardial infarction, or pulmonary embolism. The same word can mean treatment or disaster depending on the situation. That is why artificial clotting technology requires strict safety verification, as much as it inspires expectation.
The first issue to verify is location. An artificial clot must work only at the wound site where it is needed. If the gel seals the wound and then part of it breaks away and travels through the bloodstream, it could become dangerous. Researchers must determine whether it can become an embolus that blocks blood vessels, whether it is safe when it breaks down into smaller pieces, how long it remains in the body, and how it is removed. A hemostatic agent must be strong, but it cannot be strong without limit. After it stops the bleeding, it must disappear appropriately in step with the recovery process.
The second issue is immune response. Red blood cells are cells that naturally exist in the body, but if their surface proteins are chemically linked or altered, it is not yet clear how the body will recognize them. Using autologous blood can reduce this burden, but in emergencies the autologous method may not always be possible. If donor blood is used, questions of blood type, infection risk, storage stability, and immune compatibility follow. Reports noted that the researchers did not observe signs of major organ toxicity or dangerous immune responses in animal experiments, but application to humans will require much broader and longer verification.
The third issue is interaction with the clotting system. Human blood clotting is complex. The same material may not work in the same way in patients taking anticoagulants, patients with liver disease, patients with cancer, elderly patients, pregnant patients, or severely injured trauma patients whose clotting status has changed. In some patients, it may not be strong enough. In others, it may act too strongly. Hemostatic technology must be tested not against an average body, but against the many kinds of bodies that actually arrive in emergency rooms.
The fourth issue is recovery. A good hemostatic agent does not end its role by stopping blood. It must create an environment in which the wound can heal. If a material that is too rigid remains between tissues for too long, it can interfere with healing and may cause inflammation. If it disappears too quickly, bleeding may begin again. The reason click clotting research also mentions the possibility of tissue regeneration lies in this point. Hemostasis and regeneration are not separate processes. From the moment bleeding stops, the body begins repairing damaged tissue. If a hemostatic material does not interfere with this repair process and instead supports it, its value becomes much greater.
These questions do not diminish the significance of the research. Rather, they are the necessary gateways through which the technology must pass before it can become real medicine. The important task of early research is to open the door of possibility. The next stages are safety, reproducibility, manufacturing standardization, mass production, storage, regulatory approval, and clinical trials. A single paper does not immediately become a treatment. Technologies related to blood and clotting must be verified even more conservatively, because small variables can produce large consequences.
Even so, the reason this research is fascinating is clear. It is not arguing that we should accept danger. It shows a new path beyond the limits of hemostatic technology while still requiring that risks be understood. There are already many hemostatic agents in medical practice, but severe bleeding still threatens lives. Because no perfect technology exists, new approaches are needed. Click clotting is one such approach. It carries the imagination that red blood cells can become not merely oxygen-carrying cells but structural materials that seal wounds when needed. That imagination is the greatest strength of the study.
A Biomaterials Revolution Contained in a Drop of Blood
Click clotting is a hemostatic technology, but in a broader sense it is one scene in the larger story of biomaterials. Biomaterials are materials that come into contact with tissues, cells, or organs inside or outside the body and help treatment. Artificial joints, cardiac stents, sutures, artificial skin, drug-delivery gels, and scaffolds for tissue engineering all belong to this category. In the past, biomaterials research mainly focused on finding materials that could enter the body without causing major problems. It was important for a material to avoid rejection, have low toxicity, and remain durable. But recent biomaterials are becoming more active. They are evolving into “working materials” that produce specific reactions inside the body, regulate cellular behavior, and induce tissue regeneration.
Click clotting belongs to this trend. It is not simply a material placed on top of a wound. It is a material that reacts with cells in the blood to create a new structure. The environment of flowing blood, the cell surface, protein binding, tissue adhesion, and the clotting process are all connected. The importance of this technology lies in its use of a familiar cell, the red blood cell, in a new way. We think we know red blood cells very well, but the life sciences continue to discover new functions in familiar objects. The red blood cell, once understood mainly as an oxygen carrier, is now being reinterpreted as a central material for biological structures.
This change is connected to a broader trend in medical technology. Modern medicine is increasingly moving from “static materials” toward “dynamic systems.” Drugs are no longer simply chemicals that enter the body and act; they are becoming precise signals aimed at specific cells and tissues. Artificial organs are no longer mere substitutes; they are developing into structures where cells and materials function together. Medical adhesives, too, are changing from simple glues into smart materials that can work and degrade even in wet tissues and blood.
The technology for stopping bleeding is following the same path. In the past, hemostasis was largely a technology of pressing and blocking. The future of hemostasis may become a technology that attaches, withstands pressure, integrates, and supports recovery. It may involve materials that organize blood cells at the wound site, bind with fibrin, adhere to tissue, and are eventually absorbed into the body’s healing process. This is no longer simply a hemostatic agent. It is a convergent technology where emergency medicine, regenerative medicine, materials engineering, and hematology meet.
Blood is an especially accessible biological material. It can be obtained from a patient relatively easily and already contains cells and proteins that perform essential functions in the body. If blood can be rapidly processed into therapeutic material in the field, many medical scenes could change. A patient’s own blood could be used in more refined ways to seal wounds, support tissue recovery, and deliver drugs. Of course, this would require automated equipment, standardized manufacturing processes, and safe reaction conditions. But the direction is clear. It is medicine that uses the body’s own materials again for the body’s treatment.
What matters here is not the spectacle of technology but medical accessibility. If advanced technologies remain only in major hospitals, the range of lives they can save will be limited. By contrast, if they develop into safe, simple, and portable forms, they could become tools for reducing gaps in emergency care. Rapid hemostatic technology has even greater meaning in places where access to transfusion and surgery is limited, such as rural regions, disaster sites, battlefields, and medical settings in developing countries. A biomaterials revolution does not end with a laboratory paper. It becomes a true medical innovation only when it can be used in the most vulnerable settings.
The message of this research is therefore broader. Blood is not merely a liquid. It contains the basic functions of life: oxygen transport, immunity, clotting, and recovery. If those functions can be understood and precisely adjusted when needed, we can design faster and stronger treatments by using materials already within the body. Click clotting is a small window into that possibility.
Why Battlefield and Disaster Medicine Are Paying Attention
Whenever a new hemostatic technology appears, battlefield medicine and disaster medicine pay close attention for a clear reason. The most dangerous bleeding often occurs in the harshest environments. Explosions, gunshot wounds, traffic accidents, building collapses, industrial disasters, and natural disasters can all involve severe bleeding while medical resources are scarce. Treatment does not take place in a brightly lit emergency room equipped with instruments, but amid dust, noise, and confusion. Medical personnel are few, patients are many, and transport times are long. In these environments, fast and strong hemostatic technology can change survival rates.
The history of battlefield medicine is also a history of the development of hemostatic technology. In the past, tourniquet use was sometimes restricted out of concern that it could worsen tissue injury. But as deaths from uncontrolled massive bleeding continued, proper tourniquet use became an essential survival intervention in modern battlefield medicine. Hemostatic gauze and compression dressings developed for the same reason. All of these tools are meant to stop bleeding outside the hospital. If click clotting develops into an actual field-ready technology, it could become the next stage in this lineage.
Of course, exaggeration must be avoided when imagining battlefield use. Click clotting does not mean that such a technology can immediately be placed in every soldier’s first-aid kit. Storage conditions, preparation procedures, administration methods, side-effect management, and training levels must all be resolved. If it is a blood-based technology, refrigeration or blood-type management may be required. If it uses a chemical reaction, the procedure must be standardized. On a battlefield, even a small mistake can lead to great danger. Therefore, for actual use in military medicine, the technology must be extremely simple and robust.
The same is true in disaster medicine. When a large-scale accident occurs, hospital systems are pressured by a sudden influx of patients. If bleeding can be controlled at the scene, the likelihood of keeping severely injured patients alive until they reach the hospital increases. Internal bleeding in the abdomen or chest, where external pressure is difficult, remains a particularly serious problem. If artificial clotting technology someday develops into injectable, patch, gel, spray, or other forms, it could offer new alternatives even for wounds that are difficult to compress.
The operating room is also an important area of application. In trauma surgery or organ resection, the time needed to stop bleeding affects the stability of the entire operation. Continued bleeding clouds the surgical field, increases the need for transfusion, and worsens the patient’s body temperature and clotting function. Faster hemostasis may reduce surgical time and complications. Various hemostatic agents are already used in operating rooms, but there is always a need for materials that are stronger and adhere better to tissue. That is why early results showing that click clots performed better than existing natural clots are attracting attention.
But the most important question is, “Who needs this first?” This technology is not necessary for every wound. Existing hemostatic methods are enough for a paper cut or a minor injury. Technologies such as click clotting become meaningful in life-threatening bleeding, in patients with insufficient natural clotting, in bleeding that is difficult to control during surgery, and in situations where existing hemostatic agents are inadequate. To evaluate the value of the technology properly, the target of application must be narrowed accurately. It is more realistic to see it not as an all-purpose agent that solves every problem, but as a high-performance tool that buys time in the most dangerous bleeding situations.
In that sense, this research invites us to think about the future of emergency medicine. In the future, emergency care is likely to move beyond simply transporting patients to hospitals. It may begin advanced treatment before the patient reaches the hospital. Portable ultrasound, on-site blood testing, telemedicine, drone delivery, artificial-intelligence triage, and automatic infusion devices are already changing the boundaries of emergency medicine. If hemostatic technologies like click clotting are combined with these developments, the level of medical care outside the hospital may rise even further. The first life-saving treatment may begin not at the hospital door, but at the accident scene.
The Future of the Technology Depends on Trust, Not Speed Alone
There are two attitudes to avoid when looking at click clotting research. One is excessive optimism. The phrase “stops bleeding in five seconds” is powerful, but the technology has not yet become a treatment widely used in humans. Animal experiments and early biomaterials studies are stages that show possibility. Many steps remain before actual clinical application. Safety, efficacy, manufacturing processes, regulatory approval, cost, and suitability for medical settings must all be verified. In science, possibility is a starting line, not a finish line.
The other attitude is excessive cynicism. The fact that the research is still at an early stage does not mean its significance should be minimized. Medical innovation often begins with this kind of small conceptual shift. At first, it is a gel in the laboratory, a result in an animal experiment, and a figure measured under limited conditions. But if there is a new principle inside it, follow-up research refines that principle into a safer and more practical form. The idea of using blood cells as structural materials has strong research significance. Even if it does not immediately become a treatment, it can help broaden the direction of hemostatic technology.
Future hemostatic technologies may develop in several directions. First, faster preparation. To be used in the field, the process of drawing blood and triggering the reaction must be simple. Second, safer degradation. After the bleeding is stopped, it must be predictable how the material disappears inside the body. Third, more precise control of location. It must work only at the wound site and must not cause unnecessary clotting inside blood vessels. Fourth, diverse forms. Depending on the field setting and wound type, it may develop into injectable, patch, spray, or surgical gel forms. Fifth, cost and distribution. It must be able to enter real emergency medical systems rather than remain an expensive specialized treatment.
This is where trust becomes important. In technologies that deal with life, reliable repeatability matters more than astonishing speed. What is needed is not one successful experiment, but stability that works similarly across thousands of varied conditions. It must work safely not only in young and healthy experimental animals, but also in complex bodies like those of real patients. Because bleeding-control technology is used in emergencies, medical teams must be able to use it without hesitation. No matter how excellent a technology may be, if it cannot be trusted in the field, it will be difficult for it to become a life-saving tool.
Ethical questions also follow. How should donated blood be used when making blood-based biomaterials? How should patient consent be handled in emergency situations? Will a technology used in battlefield medicine also spread sufficiently to civilian medicine? Will an expensive technology be concentrated only in certain countries and hospitals? Because emergency medical technologies are directly linked to life, they cannot avoid questions of access and fairness. A good technology is not simply one with strong performance. It must also be a technology that can reach the people who need it.
This topic is meaningful in the Korean medical environment as well. Korea has strengthened its trauma center system, but transport and early treatment for severely injured patients, along with regional gaps in care, remain important issues. As the population ages, more patients will be taking anticoagulants, making bleeding management after falls or accidents more important. Rapid hemostatic technology is also an area of interest in industrial settings, military medicine, and emergency care in remote or island regions. Click clotting does not mean immediate adoption in Korean medical practice, but it can be seen as a signal showing where next-generation emergency medical technologies are heading.
In the end, the real meaning of this research is broader than a single product. The way bleeding is stopped is changing. Medicine is moving from waiting for the body to form its own clot toward designing the surface of blood cells so that they create a strong structure when needed. It is moving from materials that cover wounds toward biomaterials that work inside wounds. Emergency medicine will become faster, closer to the field, and more precise.
Five seconds is a short time. But within those five seconds lies a long set of questions. How quickly can blood be stopped? How firmly can stopped blood be held so that it does not flow again? How safe is that process for the body? And how close can this technology get to real patients in real medical settings? Click clotting research offers the first answer to these questions. It is not yet a completed treatment, but it clearly points in a direction.
Stopping bleeding has long been one of medicine’s most basic tasks. Humans have tried to stop bleeding by pressing wounds, tying limbs, stitching tissue, and applying medicine. Now a new tool is appearing before that ancient task. An artificial blood clot made by linking red blood cells. A small biological barrier formed in seconds. It is not merely a curious laboratory technology, but a possibility that could change the way emergency medicine handles life and time.
The technology that stops bleeding is ultimately a technology that gives time back. It gives patients time to reach the hospital, medical teams time to locate the injury, the body time to begin recovery, and life time to endure again. Click clotting still has many gates of verification to pass through, but beyond those gates lies a new medical landscape. At the moment blood begins to flow, medicine no longer merely waits. Now medicine is trying to seize the cells within blood and build a wall to protect life.
Reference
Nature. “Engineered blood clots stop bleeding in seconds.” April 29, 2026.
Nature. “Synthetic blood clots snap cells together to staunch bleeding — fast.” April 29, 2026.
McGill University. “McGill researchers engineer faster, more effective blood clots.” April 29, 2026.